Table of Contents ( Harvard Study )
INTRODUCTION
The number that stopped the medical world cold was 67.
Not 67 patients. Not 67 doctors. Sixty-seven percent — the accuracy rate at which an AI model diagnosed real emergency room patients in a Harvard study published in the prestigious journal Science on May 3, 2026.
The two human doctors in the same study? They scored 55 percent and 50 percent.
Same cases. Same patient records. Same information. Different results — and the AI won.
Harvard Medical School and Beth Israel Deaconess Medical Center ran one of the most carefully designed head-to-head studies in the history of medicine and technology. They put OpenAI’s reasoning model against real internal medicine physicians on 76 actual emergency room cases from a Boston hospital. They made the test as honest as possible. No preprocessing. No clean data. No shortcuts. Just the raw, messy, incomplete information that doctors see in the first chaotic minutes when a patient arrives.
The AI still won.
What the findings mean — for patients, for doctors, for hospitals, and for every country where doctors are in short supply — is now one of the most important conversations in medicine.
Also Read…. >> Google and Blackstone Confirmed a $25 Billion AI Deal Today That Could Change Cloud Computing Forever
BACKGROUND
Medicine is one of the last places most people expected AI to arrive first.
For years, the conversation about AI and jobs focused on accountants, data entry clerks, customer service agents, and truck drivers. Medicine felt different. It felt human. A doctor looks at you. Asks questions. Reads your face. Notices things no machine could notice.
That assumption has been quietly eroding for several years. But the Harvard study published in May 2026 has made it impossible to ignore.
To understand the full weight of what the study found, you have to understand what diagnosis actually involves at the emergency room triage stage — the moment a patient first arrives and the clock starts ticking.
A triage nurse takes basic measurements: blood pressure, pulse, temperature, oxygen levels. The patient or a family member gives a brief history. A note goes into the electronic medical record. Then a doctor reads that note — often in under two minutes, while managing several other patients simultaneously — and makes an initial call: What might this be? What tests should be ordered? How urgent is this?
This is exactly the scenario the Harvard team replicated. They took 76 real anonymized cases from the Beth Israel Deaconess emergency department in Boston. These were not curated cases chosen for clarity. They were raw admissions — the messy, incomplete, sometimes contradictory records that reflect what real emergency medicine actually looks like.
Two internal medicine attending physicians — experienced doctors — were given the same records. So was OpenAI’s o1 model, the company’s reasoning model capable of working through problems step by step before arriving at a conclusion.
Then two other physicians — not involved in the original diagnoses — assessed all the results blind. They did not know which answers came from humans and which came from the AI.
The study was published in Science — one of the most rigorous peer-reviewed journals in the world. Its lead researchers came from Harvard Medical School, Beth Israel Deaconess Medical Center, and Stanford University. This was not a startup press release or a tech company’s self-published report. It was the medical establishment, running the test on its own terms, publishing in its own journals.
The result landed like a stone in still water.
Also Read…. >> ChatGPT Wrongful Death Lawsuit 2026: 3 Shocking Secrets Exposed That Killed a 19-Year-Old.

MAIN UPDATE
Here are the numbers — exactly as the study reported them.
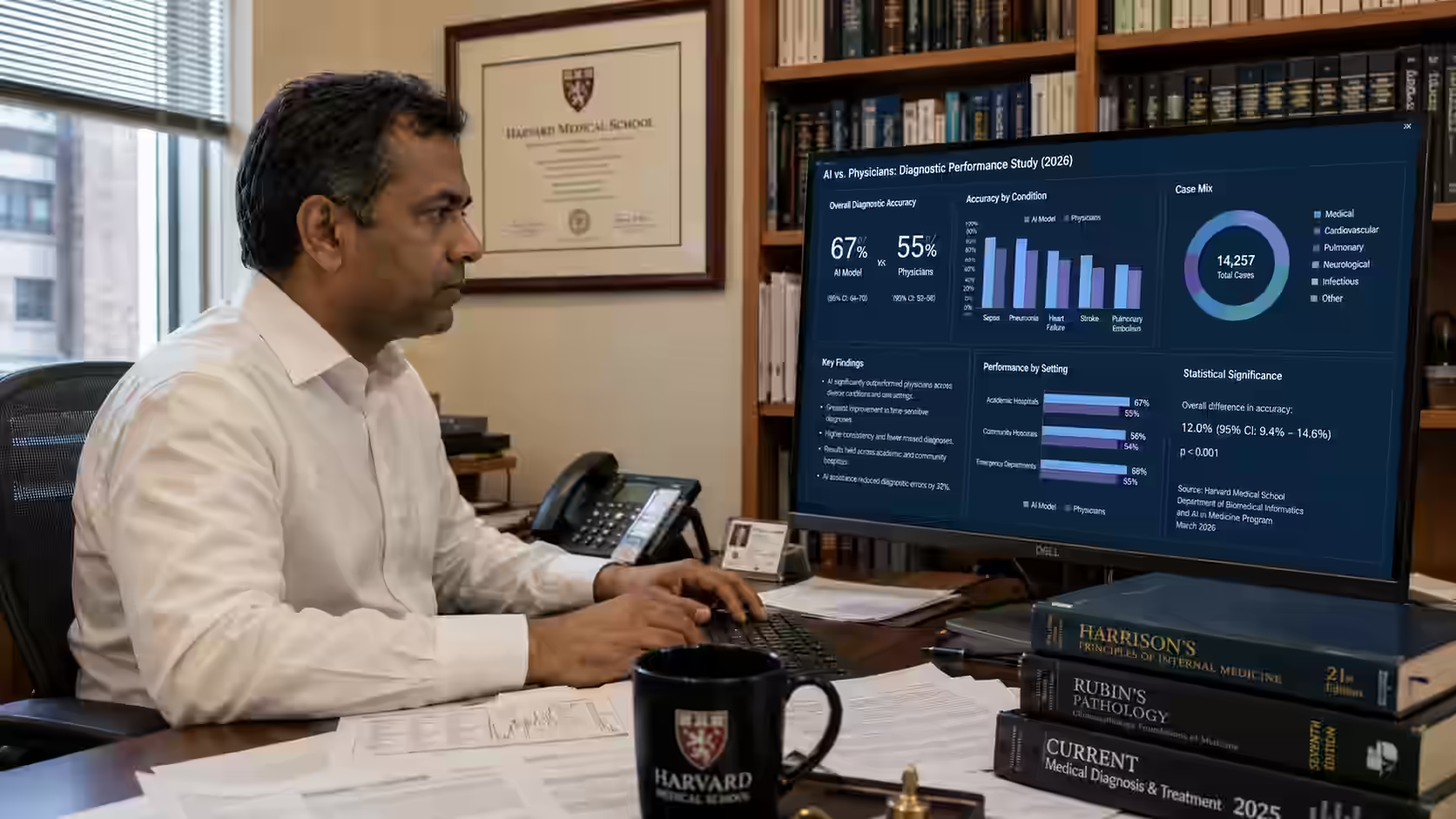
On 76 real emergency room cases, OpenAI’s o1 model achieved 67 percent diagnostic accuracy — meaning the exact or highly plausible correct diagnosis. The two human physicians scored 55 percent and 50 percent respectively. The AI was assessed as better at the most critical moment: initial triage, when the least information is available and the stakes are highest.
The study did not stop there.
When researchers gave the AI and the doctors more complete information — lab results, imaging summaries, additional clinical data — the gap narrowed. The AI reached 82 percent accuracy. The doctors reached 70 to 79 percent. The difference became smaller, but the AI still led.
Then came the number that made people genuinely uncomfortable.
In five complex long-term management cases — the kind of situations involving decisions about antibiotic regimens, palliative care, and chronic disease management — the AI scored 89 percent. The comparison group was 46 physicians who were allowed to use search engines and reference materials while answering.
Those 46 doctors, with internet access, averaged 34 percent.
The AI, with no internet access, scored 89 percent.
Arjun Manrai, senior co-author and assistant professor of biomedical informatics at Harvard’s Blavatnik Institute, put it plainly. “We tested the AI model against virtually every benchmark, and it eclipsed both prior models and our physician baselines,” he said.
The researchers were careful to note what the study did not show. The AI had no access to physical examination findings. It could not see the patient. It could not ask follow-up questions in real time. It was not being deployed in a real hospital. The study authors explicitly called for formal prospective trials before any clinical rollout.
But those caveats did not stop the medical community from paying attention.
Emergency physician Kristen Panthagani pushed back on some of the framing — noting that the comparison was against internal medicine physicians, not emergency specialists, and that the ability to guess a diagnosis from a text record is not the same as the full skill set of an ER doctor. Her point is legitimate. Diagnosing from a chart is one part of emergency medicine. The physical exam, the patient relationship, the real-time decision-making — these are not what was tested here.
What was tested was something more specific and more important than it first sounds. In the first minutes of an emergency, when the record is thin and the pressure is maximum, which intelligence — human or machine — makes better initial calls?
The answer, from this study, is the machine.
Also Read…. >> Google I/O 2026 Confirmed 7 AI Secrets Today That Could End ChatGPT’s Dominance Forever
IMPACT ANALYSIS
The study’s implications ripple outward in multiple directions — and not all of them are what you might expect.
For patients, the most immediate question is simple: if AI is already more accurate than a doctor at initial diagnosis, should patients have access to it? The honest answer is that this study does not yet justify changing clinical practice. The researchers themselves said so. But it does raise a question that health systems, insurance companies, and regulators are now actively discussing: can AI be used as a first-pass screening tool, before or alongside a doctor, to reduce the number of misdiagnoses that occur every year?
Misdiagnosis is not a minor problem. A 2023 estimate suggested that diagnostic errors contribute to approximately 800,000 deaths and permanent disabilities in the United States annually. In India, with a doctor-to-patient ratio of approximately 1 to 856 — far below the World Health Organization’s recommended 1 to 600 — the shortage of physicians is a genuine public health crisis. An AI tool that can perform initial triage accurately, without fatigue and without needing to be physically present, is not a theoretical luxury. It is a potential solution to a problem that kills people every year.
For the medical profession, the implications are more uncomfortable. Doctors have long acknowledged that AI would eventually assist in medicine. Most assumed it would assist them — handling paperwork, flagging drug interactions, reading imaging scans. The idea that it would outperform them at the core cognitive task of diagnosis is a harder reality to absorb.
For OpenAI, the study provides the most credible third-party validation of its medical capabilities to date. The company launched ChatGPT Health in January 2026, a platform that allows users to upload medical records and receive personalized health guidance. That product now serves over 40 million daily health consultations, according to OpenAI’s own figures.
The question of liability — who is responsible when an AI diagnosis is wrong — remains entirely unresolved.
Also Read…. >> Microsoft AI Chief Said 18 Months — 3 Months Later Here Is What Actually Happened

FUTURE OUTLOOK
The Harvard study is one data point — an important one, but one that sits in a rapidly changing landscape.
What the researchers called for is a prospective trial: a real-world study in which AI and human doctors operate in parallel in a live clinical environment, with patients’ outcomes tracked over time. Several hospitals in the United States and the United Kingdom are already in early planning stages for exactly this kind of study. Results from the first wave of prospective trials are expected sometime in 2027 or 2028.
If those trials confirm the accuracy findings from the Harvard study, the implications for medical training, hospital staffing, and global health access will be significant. Countries with severe doctor shortages — including large parts of Sub-Saharan Africa, South Asia, and Southeast Asia — could deploy AI diagnostic tools as a first layer of care in areas where no doctor is physically available.
In higher-income countries, the more likely near-term scenario is AI as a diagnostic partner rather than a replacement. A doctor who has the AI’s reasoning available alongside their own assessment is more likely to catch what they miss alone. Several emergency departments in the United States have already begun using AI to flag high-risk patients for faster escalation — not to replace triage decisions, but to add a second layer of attention.
The harder question is what happens in 2030 or 2035, when AI diagnostic models are three or four generations beyond o1 — the model used in this study. O1 was released by OpenAI a year before the study. OpenAI’s current models are significantly more capable. The trajectory is not pointing toward a plateau.
For medical students entering training today, the skills that will matter most are not the ones most easily replicated by a reasoning model. Clinical judgment that requires physical examination, patient communication, ethical decision-making under uncertainty, and the ability to act in real time on incomplete information — these remain distinctly human. But the cognitive task of parsing a medical record and arriving at a differential diagnosis? That gap is closing faster than most of the medical establishment expected.
Also Read…. >> Why Elon Musk’s OpenAI Trial Exposed 7 Secrets That Could Change AI Forever

EXPERT INSIGHTS
- Arjun Manrai, Senior Co-Author, Harvard Medical School (May 3, 2026): “We tested the AI model against virtually every benchmark, and it eclipsed both prior models and our physician baselines.” Manrai is an assistant professor of biomedical informatics at Harvard’s Blavatnik Institute and led the study team.
- Harvard / Beth Israel / Stanford research team (Science, May 2026): The paper explicitly states that language models have now “surpassed most existing benchmarks for clinical reasoning” — and calls for urgent formal prospective trials to determine how AI can be most effectively deployed in real clinical settings.
- Kristen Panthagani, Emergency Physician (May 2026): Called the study “an interesting AI study that has led to some very overhyped headlines.” Her specific critique: the AI was compared to internal medicine physicians, not ER specialists. “If we’re going to compare AI tools to physicians’ clinical ability, we should start by comparing to physicians who actually practice that specialty.”
- TechCrunch analysis of the study: Noted that the AI’s advantage was “especially pronounced at the first diagnostic touchpoint — initial ER triage — where there is the least information available about the patient and the most urgency to make the correct decision.” This is the moment the study authors considered most clinically significant.
- OpenAI (January 2026, ChatGPT Health launch): Stated that ChatGPT Health serves over 40 million daily health consultations — describing it as a tool to “support, not replace, medical care.” The Harvard study provides independent academic validation of the underlying model’s diagnostic capabilities.
- Independent medical analysis (Quasa.io, May 2026): Noted that the AI models “don’t suffer from cognitive fatigue, time pressure, or the tendency to skip details that affect human performance in high-stress environments” — identifying the structural reasons why AI may consistently outperform tired doctors in controlled comparisons.
- World Health Organization data (background context): India’s doctor-to-patient ratio remains approximately 1 to 856 — significantly below the WHO recommended 1 to 600. AI diagnostic tools could address a portion of this gap in underserved regions, particularly at the initial screening level.
Also Read…. >> CEO Deleted The ChatGPT Chat — The Same Deleted Chat Exposed Him In Court
KEY TAKEAWAYS
- A Harvard Medical School study published in Science on May 3, 2026 found that OpenAI’s o1 reasoning model outperformed two internal medicine physicians at diagnosing real emergency room patients — 67% accuracy versus 55% and 50% respectively.
- The AI performed best at the most critical moment: initial triage, when the least information is available and the pressure to make the right call is highest.
- In complex long-term management cases, the AI scored 89% accuracy — compared to 34% for 46 physicians who were allowed to use search engines and reference materials during the test.
- The study used 76 real anonymized cases from Beth Israel Deaconess Medical Center in Boston, with no data preprocessing — the AI and doctors received exactly the same raw information from electronic health records.
- The researchers explicitly stopped short of recommending clinical deployment, calling instead for formal prospective trials before AI is used in real patient care decisions.
- Critics, including emergency physician Kristen Panthagani, noted that the comparison group were internal medicine physicians — not ER specialists — and that chart-based diagnosis does not capture the full scope of emergency medicine skills.
- OpenAI’s ChatGPT Health, launched in January 2026, already serves over 40 million daily health consultations — the Harvard study provides the most credible independent validation of the underlying model’s diagnostic capabilities to date.
- For countries like India — where doctor shortages are severe and millions of patients never reach a physician in time — AI diagnostic tools represent a potential public health intervention at a scale
- that traditional healthcare expansion cannot match.
Also Read…. >> Anthropic India’s CEO Revealed 5 Predictions That Could Change India Forever by 2030
CONCLUSION
A number from a hospital in Boston has changed a question the medical world thought it had more time to answer.
For decades, doctors have asked: will AI eventually be as good as us? The Harvard study published in May 2026 suggests the question has already moved on. In at least one critical area — parsing a medical record and arriving at the right initial diagnosis — AI is not catching up to doctors. It has passed them.
That does not mean AI should replace doctors. The researchers themselves said it clearly. But it does mean the conversation about how AI fits into medicine is no longer theoretical. It is urgent, it is real, and the data behind it has just been published in one of the world’s most respected scientific journals.
For patients, the question is not whether they trust AI. It is whether they can afford to ignore a tool that, in this study, was right more often than the doctor.
What do YOU think — would you trust an AI diagnosis over your doctor’s? Drop your thoughts below. Share this with one person who works in healthcare or has a family member who does. Follow AI Today’s News to stay ahead every day.